Screenshots from a real local session.
The provider portal, running against the actual prover and verifier services on localhost. These are real screenshots, not mockups.
Patient intake
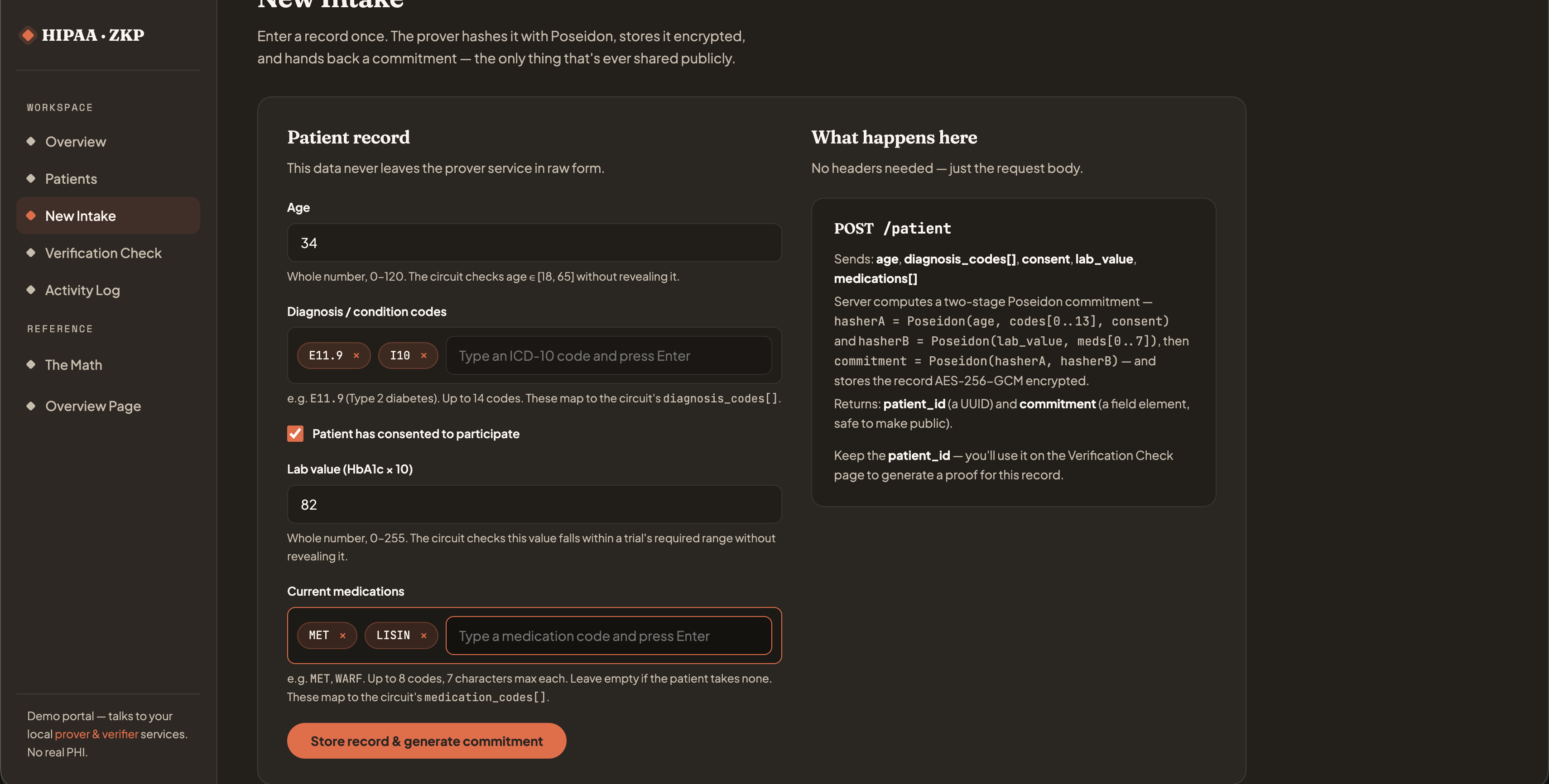
The intake form now also takes a lab value and a medication list, all hashed into the two-stage Poseidon commitment before the record is stored.
Dashboard overview
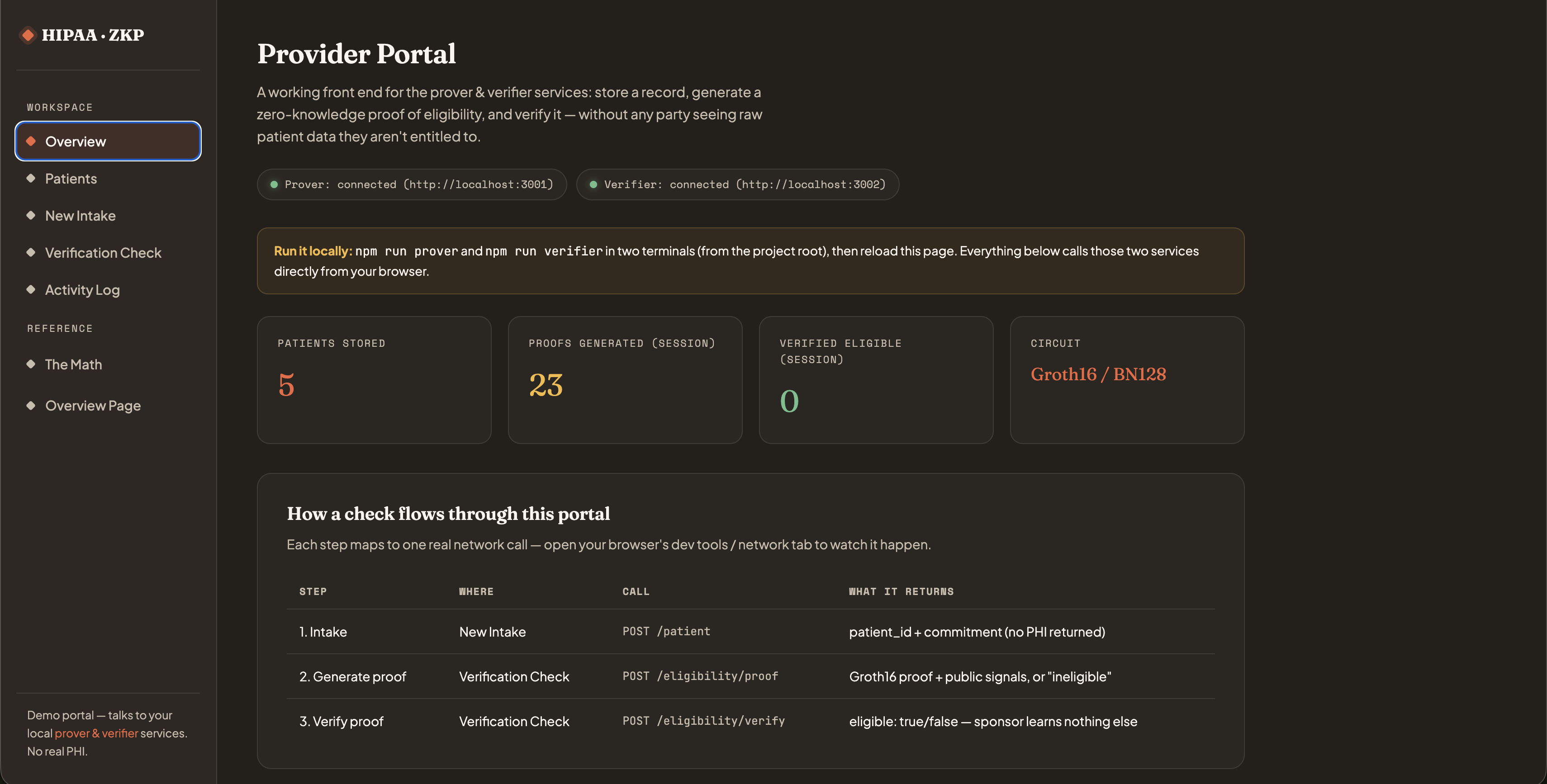
Both services connected (ports 3001/3002), with live counts of patients stored and proofs generated this session.
Patient roster
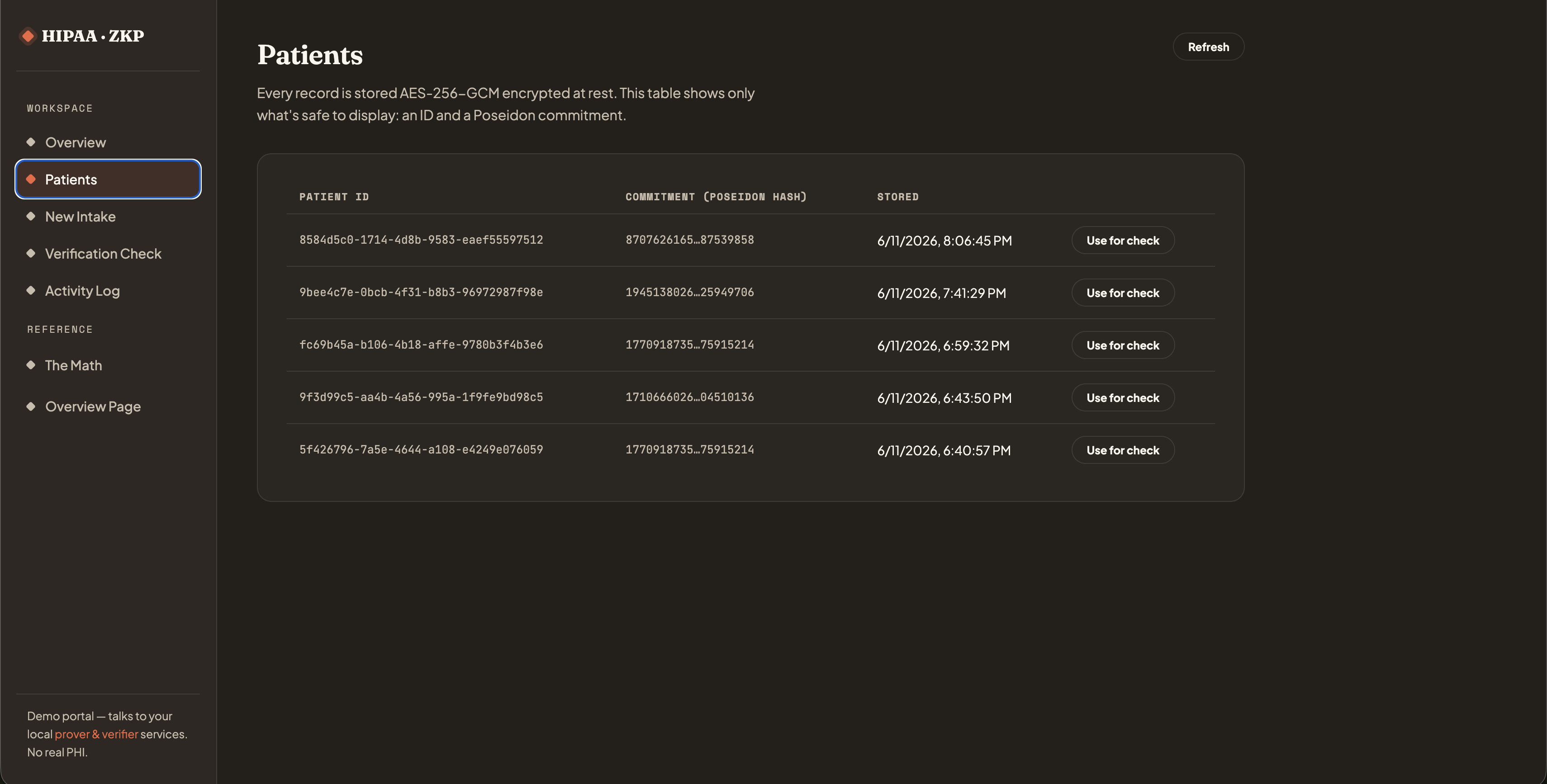
Only an ID, a Poseidon commitment, and a timestamp are ever shown. The encrypted record itself never appears here.
A rejected check
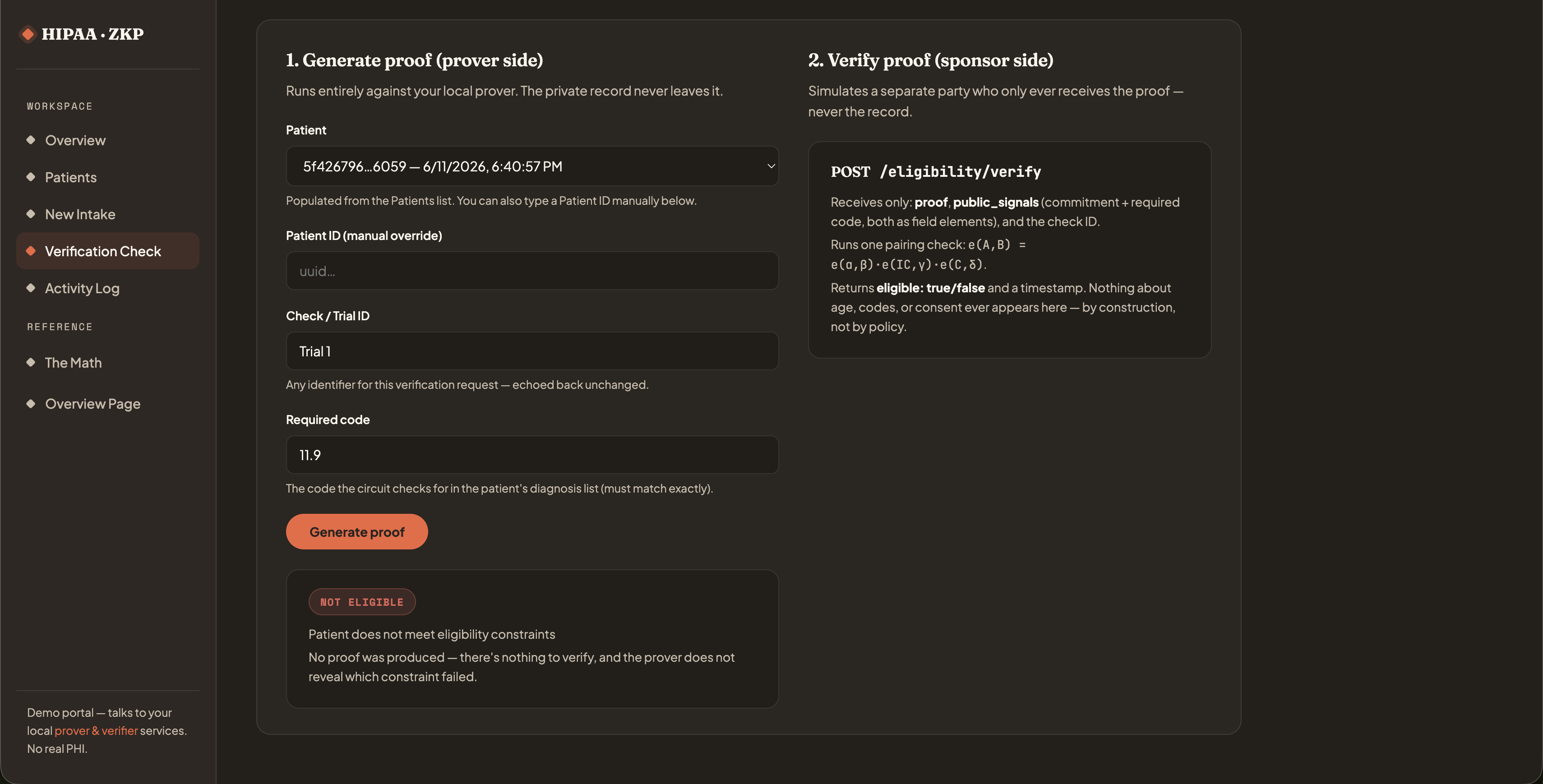
When a record doesn't satisfy the circuit, the prover returns "not eligible" with no proof and no explanation of which rule failed.
A successful proof
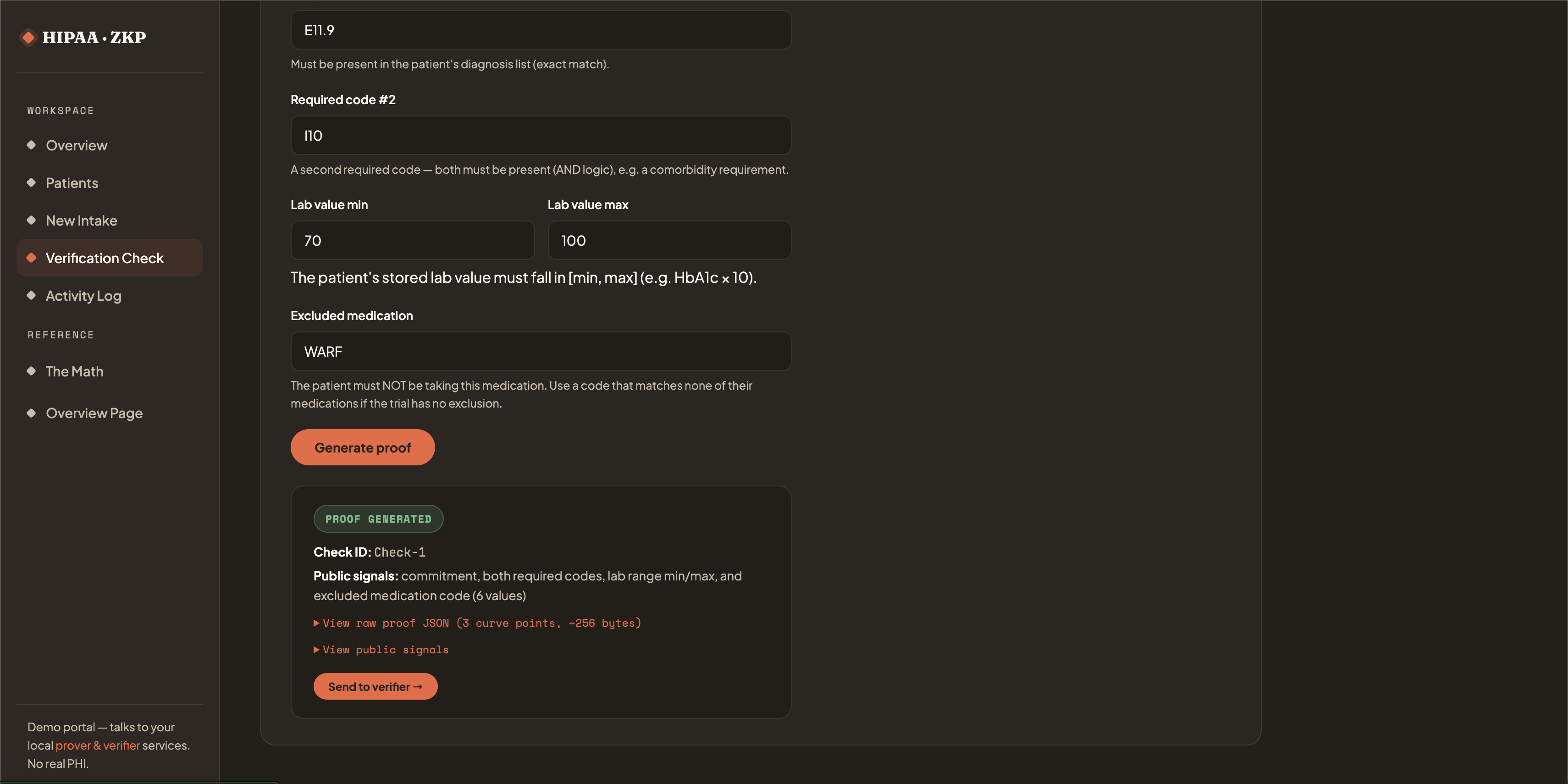
Same flow, but this record satisfies all eight constraints (both diagnosis codes, the lab range, the medication exclusion, age, and consent), so it produces a real Groth16 proof and six public signals, ready to hand to the verifier.
Activity log
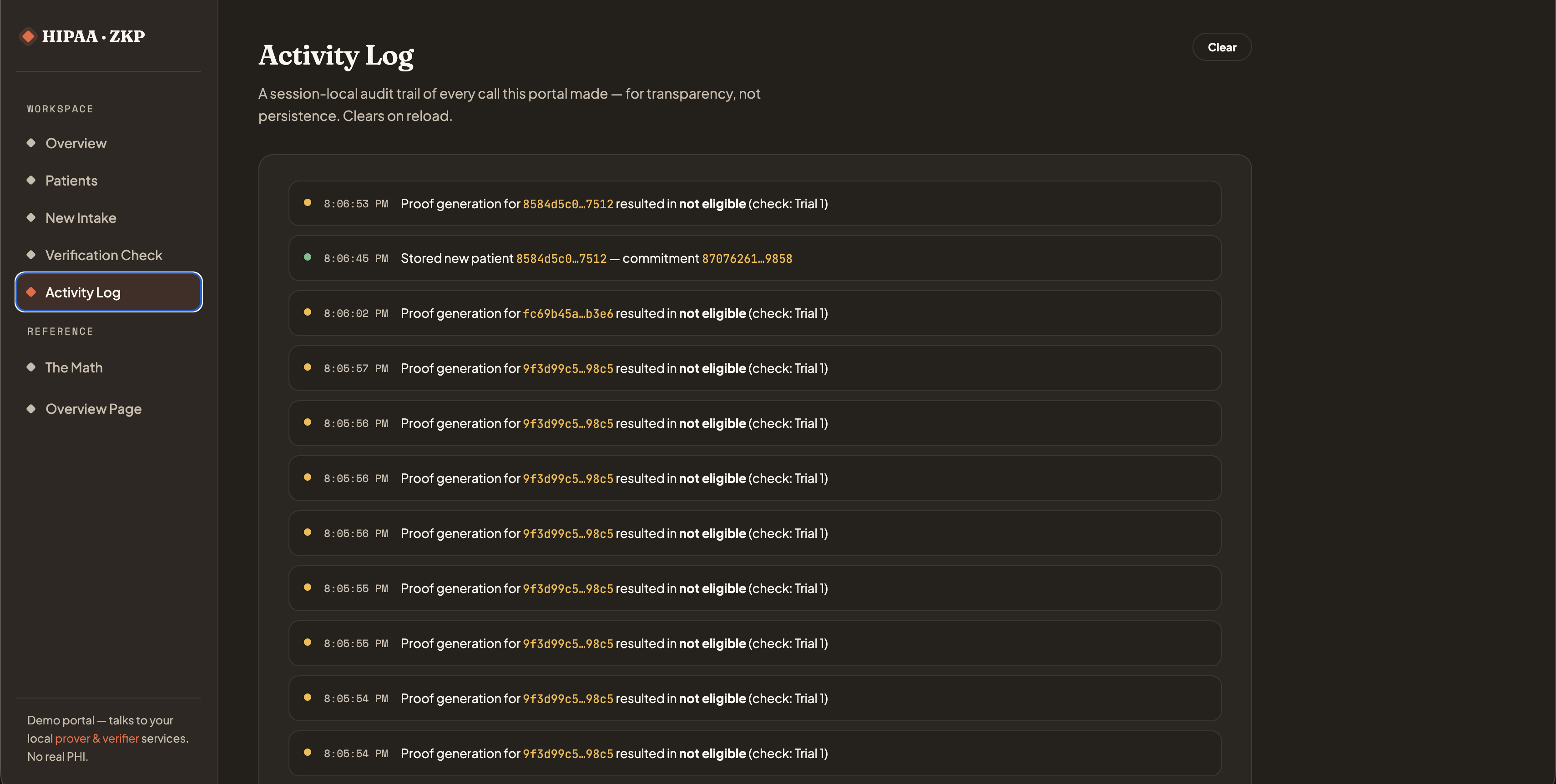
Every proof request made during the session, success or not, ends up here as a session-local audit trail.